The Four-Stage Engagement Model: A New Paradigm for Mental Health and Housing Services
The Four-Stage Engagement Model: A New Paradigm for Mental Health and Housing Services
Authors
Frederick Shack, LMSW1,4
Mardoche Sidor, MD1,2,3
Jose Cotto, LCSW1,5
Karen Dubin, PhD, LCSW2,4
Gary Jenkins, MPA1
Lesmore Willis Jr, MPA, MHA1
Affiliations
1Urban Pathways, New York, NY
2SWEET Institute, New York, NY
3Columbia University Center for Psychoanalytic Study and Research, New York, NY
4Columbia University, Department of Social Work, New York, NY
5New York University, Department of Social Work, New York, NY
Correspondence concerning this article should be addressed to Mardoche Sidor, MD, Urban Pathways, at msidor@urbanpathways.org
Abstract
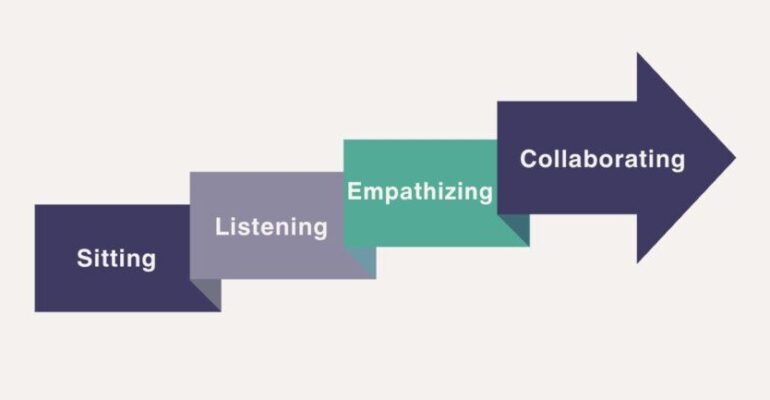
Engagement is the cornerstone of effective mental health and housing services, yet it is often misunderstood or narrowly defined as client willingness to participate. We present the Four-Stage Engagement Model — Sitting, Listening, Empathizing, and Collaborating — a framework developed through practice at Urban Pathways. Rooted in motivational interviewing, trauma-informed care, and the stages of change, this model reframes engagement as a staff-driven responsibility rather than a client deficit. Each stage builds sequentially: presence (sitting), active listening (listening), corrective emotional experience through unconditional positive regard (empathizing), and tailored partnership aligned with stage of change (collaborating). We argue this model provides a replicable roadmap for clinicians and staff across mental health, housing, and community-based settings, improving trust, adherence, and outcomes.
Keywords
Engagement, Trauma-Informed Care, Motivational Interviewing, Corrective Emotional Experience, Unconditional Positive Regard, Stages of Change, Supportive Housing, Mental Health Services
Introduction
Engagement has long been recognized as a predictor of treatment outcomes across psychiatry, psychology, and social services (Priebe et al., 2010). Yet frontline staff frequently describe clients as “non-compliant” or “unengaged,” reflecting a systemic misattribution of responsibility (Stanhope et al., 2016). Individuals experiencing homelessness, serious mental illness, substance use disorders, and trauma histories face complex relational barriers to trust and participation (Drake et al., 2020).
The Four-Stage Engagement Model reframes engagement as a staff-led, relational process, moving away from compliance-oriented frameworks. Developed by Urban Pathways, this model integrates evidence-based principles from motivational interviewing (Miller & Rollnick, 2013), trauma-informed care (SAMHSA, 2014), Rogers’ unconditional positive regard (Rogers, 1957), corrective emotional experience (Alexander & French, 1946), and the transtheoretical model of change (Prochaska & DiClemente, 1984).
Theoretical Framework
The model consists of four stages:
- Sitting – Derived from research on co-regulation and presence, the act of sitting without agenda reduces arousal and conveys psychological safety (Porges, 2011).
- Listening – Active listening enhances therapeutic alliance, a consistent predictor of outcomes across modalities (Norcross & Wampold, 2019).
- Empathizing – Beyond cognitive empathy, empathizing here entails corrective emotional experience (Alexander & French, 1946) and unconditional positive regard (Rogers, 1957), both essential for healing relational trauma.
- Collaborating – Rooted in motivational interviewing and the stages of change, collaboration requires tailoring engagement strategies to the individual’s stage of change (DiClemente et al., 2004).
This layered framework acknowledges that trust and collaboration are not immediate but built through sequenced, evidence-based interactions.
Application/Analysis
At Urban Pathways, frontline staff are piloting the model through reflective checklists and supervision. Case examples show how shifting from “the resident is unengaged” to “we need to re-engage this person differently” transformed practice. For example:
- A resident labeled “resistant” responded positively once staff prioritized sitting in shared spaces, signaling availability without pressure.
- Another resident progressed when staff moved from listening for goals (“Tell me what a good day would look like for you”) to empathizing through validating his lived experience, which served as a corrective emotional moment.
- Collaboration emerged when staff tailored interventions to stages of change — providing information in precontemplation, supporting planning in preparation, and celebrating small wins in maintenance.
Early implementation suggests the model can reduce staff frustration, increase trust, and support resident-driven progress.
Implications
The Four-Stage Engagement Model has broad implications for:
- Practice: Provides a replicable roadmap for staff at varying levels of training.
- Training: Aligns with trauma-informed and motivational interviewing curricula, enhancing fidelity.
- Supervision: Offers a reflective tool for supervisors to support staff development.
- Policy: Shifts systemic discourse from compliance to engagement, challenging stigmatizing labels.
- Research: Opens pathways for measuring outcomes linked to engagement stages, such as trust, alliance, and housing retention.
Conclusion
The Four-Stage Engagement Model offers a structured, evidence-informed framework for reframing engagement in mental health and housing services. By centering staff responsibility, it empowers organizations to move beyond compliance-based paradigms toward healing, relational, and collaborative care.
References
- Alexander, F., & French, T. (1946). Psychoanalytic therapy: Principles and application. Ronald Press.
- DiClemente, C. C., Schlundt, D., & Gemmell, L. (2004). Readiness and stages of change in addiction treatment. The American Journal on Addictions, 13(2), 103–119.
- Drake, R. E., Bond, G. R., & Becker, D. R. (2020). Individual placement and support: An evidence-based approach to supported employment. Oxford University Press.
- Miller, W. R., & Rollnick, S. (2013). Motivational interviewing: Helping people change (3rd ed.). Guilford Press.
- Norcross, J. C., & Wampold, B. E. (2019). Relationships and responsiveness in the psychological treatment of trauma: The transtheoretical paradigm. Psychotherapy, 56(3), 421–430.
- Porges, S. W. (2011). The polyvagal theory: Neurophysiological foundations of emotions, attachment, communication, and self-regulation. Norton.
- Priebe, S., Watts, J., Chase, M., & Matanov, A. (2010). Processes of disengagement and engagement in assertive outreach patients: Qualitative study. British Journal of Psychiatry, 197(5), 423–429.
- Prochaska, J. O., & DiClemente, C. C. (1984). The transtheoretical approach: Crossing traditional boundaries of therapy. Dow Jones-Irwin.
- Rogers, C. R. (1957). The necessary and sufficient conditions of therapeutic personality change. Journal of Consulting Psychology, 21(2), 95–103.
- Substance Abuse and Mental Health Services Administration (SAMHSA). (2014). SAMHSA’s concept of trauma and guidance for a trauma-informed approach. HHS Publication.
This article is part of a collaboration between SWEET Institute and Urban Pathways

Read the full scientific version HERE




